distinguishing long-term gastrointestinal conditions
introduction
There is significant overlap in presenting symptoms across different lower-GI conditions (Table 1).
Key similarities and distinctions include:
•
Blood with bowel motions and loose or watery bowel motions are the most common presenting symptoms with ulcerative colitis (UC).
•
Fatigue and abdominal pain are the most common presenting symptoms with Crohn’s disease (CD).
•
Coeliac disease rarely presents with blood or mucous in bowel motions.
•
Blood with bowel motions is not a feature of IBS.
•
Fatigue is very common across IBD, coeliac disease and IBS.
1/5
Blood with bowel motions and loose or watery bowel motions are the most common presenting symptoms with ulcerative colitis (UC)
2/5
Fatigue and abdominal pain are the most common presenting symptoms with Crohn's disease (CD)
3/5
Coeliac disease rarely presents with blood or mucous in bowel motions
4/5
Blood with bowel motions is not a feature of IBS
5/5
Fatigue is very common across IBD, coeliac disease and IBS
Table 1. Symptom prevalence by disease (%)¹⁻⁵
Symptom
UC
UC
CD
CD
UC+CD
UC+CD
CoD
CoD
IBS
IBS
Blood with bowel motions
Urgency of bowel motions
Loose/watery bowel motions
Increased frequency of bowel motions
Tiredness/fatigue
Abdominal pain
Mucous with bowel motions
Blood from anus (fresh/not mixed with bowel motions)
Anxiety about distance to bathroom
Cramping with bowel motion
Sense of incomplete evacuation after bowel motion
Fissures, abscesses or fistulae
87
83
87
80
74
68
68
60
59
67
73
-
45
64
70
62
81
80
37
32
39
66
63
10
66
73
78
71
77
74
52
46
49
66
68
-
Rare
-
56
56
41-82
77
Uncommon
Rare
-
-
-
-
Not a feature
Very common
Very common
Very common
Very common
Universal
Very common
Not a feature
-
Common
Common
-
Notes: Highlights show the five most reported symptoms in each condition. Average alarm symptoms for IBD are urgency, loose/watery bowel motions, increased frequency, tiredness/fatigue and abdominal pain. Blank cells do not imply absence of this symptom in this condition, only absence of data in the cited studies.
CoD=coeliac disease; CD=Crohn’s disease; IBS=irritable bowel syndrome; UC=ulcerative colitis.
Table 1. Symptom prevalence by disease (%)¹⁻⁵
Symptom
UC
UC
CD
CD
UC+CD
UC+CD
CoD
CoD
IBS
IBS
Blood with bowel motions
Urgency of bowel motions
Loose/watery bowel motions
Increased frequency of bowel motions
Tiredness/fatigue
Abdominal pain
Mucous with bowel motions
Blood from anus (fresh/not mixed with bowel motions)
Anxiety about distance to bathroom
Cramping with bowel motion
Sense of incomplete evacuation after bowel motion
Fissures, abscesses or fistulae
87
83
87
80
74
68
68
60
59
67
73
-
45
64
70
62
81
80
37
32
39
66
63
10
66
73
78
71
77
74
52
46
49
66
68
-
Rare
-
56
56
41-82
77
Uncommon
Rare
-
-
-
-
Not a feature
Very common
Very common
Very common
Very common
Universal
Very common
Not a feature
-
Common
Common
-
Notes: Highlights show the five most reported symptoms in each condition. Average alarm symptoms for IBD are urgency, loose/watery bowel motions, increased frequency, tiredness/fatigue and abdominal pain. Blank cells do not imply absence of this symptom in this condition, only absence of data in the cited studies.
CoD=coeliac disease; CD=Crohn’s disease; IBS=irritable bowel syndrome; UC=ulcerative colitis.
Table 1. Symptom prevalence by disease (%)1-5
Symptom
UC
UC
CD
CD
UC+CD
UC+CD
CoD
CoD
IBS
IBS
Symptom
Blood with bowel motions
Urgency of bowel motions
Loose/ watery bowel motions
Increased frequency of bowel motions
Tiredness/ fatigue
Abdominal pain
Mucous with bowel motions
Blood from anus (fresh/ not mixed with bowel motions)
Anxiety about distance to bathroom
Cramping with bowel motion
Sense of incomplete evacuation after bowel motion
Fissures, abscesses or fistulae
UC
87
83
87
80
74
68
68
60
59
67
73
-
CD
45
64
70
62
81
80
37
32
39
66
63
10
UC + CD
66
73
78
71
77
74
52
46
49
66
68
-
CoD
Rare
-
56
56
41-82
77
Uncommon
Rare
-
-
-
-
IBS
Not a feature
Very common
Very common
Very common
Very common
Universal
Very common
Not a feature
-
Common
Common
-
Notes: Highlights show the five most reported symptoms in each condition. Average alarm symptoms for IBD are urgency, loose/watery bowel motions, increased frequency, tiredness/fatigue and abdominal pain. Blank cells do not imply absence of this symptom in this condition, only absence of data in the cited studies. CoD=coeliac disease; CD=Crohn’s disease; IBS=irritable bowel syndrome; UC=ulcerative colitis.
Headline goes here
Intro goes here
Irritable bowel syndrome
Click for more info
IBS is a longstanding illness with frequent abdominal discomfort and bowel symptoms that cannot be explained by any other disease. GI presentations include:
Abdominal pain or discomfort (present for at least 6 months) and relieved by defecation or associated with altered bowel frequency or stool form
Altered stool passage (straining, urgency, incomplete evacuation)
Abdominal bloating (more common in women than men)
Passage of mucus
IBS often also has extraintestinal features, including lethargy, nausea, back pain, headache or bladder symptoms. The condition rarely presents for the first time in people over 50 years old. The National Primary Care Diagnostic Pathway for Lower-GI Symptoms focuses on diarrhoea-predominant IBS (IBS-D).
The ROME criteria
A diagnosis of IBS can be supported by the ROME criteria.6 Recurrent abdominal pain on average at least 1 day a week in the past 3 months, associated with two or more of the following criteria:
•
Related to defecation
•
Associated with a change in stool frequency
•
Associated with a change in stool form (appearance)
These criteria need to be fulfilled for the past 3 months, with symptom onset at least 6 months prior to diagnosis.


Quote goes here and here and here like this??
Making a diagnosis
IBS is a positive clinical diagnosis based on characteristic symptoms and normal initial investigations, rather than a diagnosis made only after excluding all other conditions.7,8 A confident diagnosis of IBS can be made according to following symptoms:9
•
Abdominal pain
•
Bowel dysfunction
•
Bloating
The diagnosis also requires exclusion of alarm symptoms, such as unintentional weight loss, rectal bleeding or recent change in bowel function, alongside normal haemoglobin (Hb), C-reactive protein (CRP), abdominal examination and digital rectal examination (DRE). Features not typical of IBS, such as nocturnal symptoms, iron deficiency anaemia, rectal bleeding or raised inflammatory markers, should prompt reconsideration of the diagnosis and further investigation.7,8

Click for more info
Coeliac disease
Coeliac disease occurs in 1-in-100 people and is undiagnosed in two-thirds of cases. It can present in non-specific ways, involving the common symptoms of lower-GI conditions described earlier, although potential distinguishing symptoms include:
Dermatitis herpetiformis
Tooth enamel problems
Reduced bone mineral density
Unexplained subfertility or repeated miscarriages
Neurological problems such as unexplained ataxia or peripheral neuropathy
Coeliac UK focuses on fatigue, abdominal pain, nausea, anaemia and neurological symptoms as common symptoms and signs of coeliac disease in adults.10 A 40-year single-centre analysis of 1547 found GI symptoms present in approximately half of coeliac patients, including:11

24.3%
Diarrhoea
28%
Abdominal bloating
19.7%
Aphthous stomatitis
Quote goes here and here and here like this??
Risk factors for Coeliac disease include:
•
Family history, with a first-degree relative associated with a 1-in-10 risk
•
Down‘s or Turner syndrome
•
History of autoimmune conditions (e.g. type 1 diabetes or thyroid disease)
•
Iron-deficiency anemia or B12 or folate deficiency.
Yes, two-way sync keeps tasks aligned across platforms.
Inflammatory bowel disease
IBD, which includes CD and UC, often presents with common lower-GI-symptoms, especially diarrhoea, abdominal pain, rectal bleeding or weight loss. Potential distinguishing symptoms include:
Nocturnal defecation
Fevers
Recurrent/persistent anal abscesses
Extra-intestinal manifestations (EIMs) in joints, skin, eyes or perianal area
Perianal symptoms, such as fissures, abscesses or fistulae, may present early in CD, sometimes before intestinal symptoms.12-14
IBD is classically considered as a disease of young adulthood, usually presenting in people aged 18–35 years. However, there is a second spike at around 65 years, with a large Swedish study showing 23% of IBD patients to be at least 60 years old at point of diagnosis.15
Family history of IBD in a first-degree relative increases risk and should be considered during initial assessment.
Microscopic colitis
Microscopic colitis is a subset IBD distinct from CD or UD. The classical presentation is chronic watery non-bloody diarrhoea in older women (>60 years).16 Others follow a similar pattern to lower-GI CD, with faecal urgency, arthralgias, weight loss, abdominal pain, passage of stools at night and faecal incontinence.17,18 Microscopic colitis is associated with:
•
Autoimmune conditions, including coeliac disease, thyroid disorders and polyarthritis16
•
Lifestyle factors, including smoking19
•
Medications, including statins, selective serotonin reuptake inhibitors (SSRIs), proton-pump inhibitors (PPIs) and non-steroidal anti-inflammatory drugs (NSAIDs), with the latter two also associated with a rise in faecal calprotectin (FCP).17
Microscopic colitis cannot be diagnosed in primary care.
Microscopic colitis is challenging to diagnose, as it appears macroscopically normal on endoscopy and requires histological confirmation by biopsy. A normal FCP result does not exclude a diagnosis (67% sensitivity; 75% specificity20), so patients under high clinical suspicion should be referred for consideration of colonoscopy with biopsy. Many patients with undiagnosed microscopic colitis may have been through a diagnostic pathway with a colonoscopy already.18
Around 10%21 of microscopic colitis cases are self-limiting,22 but treatment with oral budesonide has been demonstrated to induce remission in between 54% to 84% of patients.23 Loperamide may be suggested for symptomatic relief; however, there is a limited evidence base for this and other treatments.
Extra-intestinal manifestations
IBD may have EIM (Table 2)s:24,25
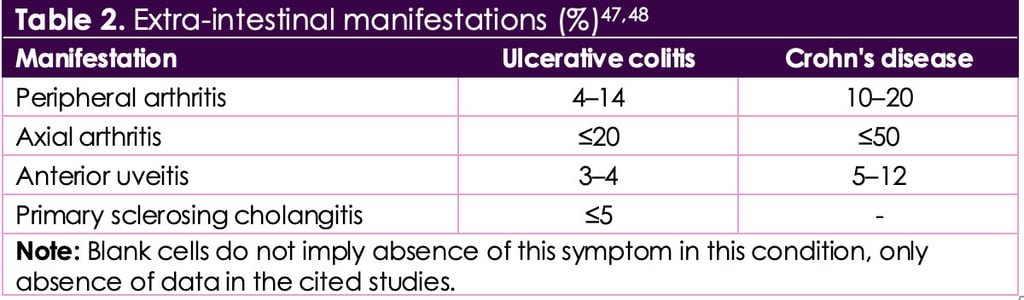
Table 2. Extra-intestinal manifestations (%)28,29
Manifestation
UC
UC
CD
CD
Manifestation
Peripheral arthritis
Axial arthritis
Anterior uveitis
Primary sclerosing cholangitis
UC
4-14
≤20
3-4
≤5
CD
10-20
≤50
5-12
-
Notes: Blank cells do not imply absence of this symptom in this condition, only absence of data in the cited studies.
•
Dependent on the definition, the prevalence of EIMs is reported to be between 6% and 47% of all patients.26
•
Patients may be affected by more than one EIM, with over 20% of IBD patients reporting two EIMs and over 10% of patients reporting three or more.26
•
EIMs may occur before or after IBD diagnosis, with 26% of all patients with EIMs report occurrence of EIMs up to 25 months (median 5 months) before IBD diagnosis.26
•
EIMs can precede bowel symptoms, so new uveitis, inflammatory back pain, erythema nodosum or peripheral arthritis alongside GI symptoms should raise suspicion for IBD.26
In 25.8% of cases, patients presented with their first EIM before IBD was diagnosed (median 5 months, range 0–25 months), while in 74.2% of cases, the first EIM manifested itself after IBD diagnosis (median 92 months, range 29–183 months).27
First extra-intestinal manifestations of inflammatory bowel disease27

Peripheral arthritis
70.0%
Hands, wrists, knees, ankles, elbows

Aphthous stomatitis
21.6%
Mouth
Axial arthropathy/ ankylosing spondylitis
16.4%
Chest, back, hips
Uveitis
13.7%
Eyes
Erythema nodosum
12.6%
Shins
Primary sclerosing cholangitis
6.6%
Liver
Pyoderma gangrenosum
4.9%
Skin
Psoriasis
2.7%
Skin
First extra-intestinal manifestations of inflammatory bowel disease²⁷
•
70.0%
Peripheral arthritis
•
21.6%
Aphthous stomatitis
•
16.4%
Axial arthropathy/ ankylosing spondylitis
•
13.7%
Uveitis
•
12.6%
Erythema nodosum
•
4.9%
Pyoderma gangrenosum
•
2.7%
Psoriasis
HIV
Yes, two-way sync keeps tasks aligned across platforms.
HIV screening may be warranted in patients with GI symptoms, including chronic diarrhoea, depending on HIV stage:
Acute HIV infection in the first few weeks after exposure can include diarrhoea, nausea, fever, sore throat and muscle aches
Advanced HIV commonly includes persistent diarrhoea lasting more than a month, often linked to opportunistic infections
Patients continue to be diagnosed late with HIV. Review of late diagnoses showed 62% had missed opportunities for diagnosis, of which 62% were in primary care. Of these patients, 82% presented with indicator conditions, which can include chronic diarrhoea.31 GPs may miss opportunities to test for HIV due to:
•
Lack of knowledge of indicator conditions
•
Concern about causing offence to patient by suggesting an HIV test
•
Concern about consent required for test to be offered (minimum is seeking agreement to test and telling patient how result will be given).32
Patients continue to be diagnosed late with HIV. Review of late diagnoses showed 62% had missed opportunities for diagnosis, of which 62% were in primary care
fffffffx
vzzxvzvxç
fffff
zgszdgzdsbdzf
Irritable bowel syndrome
IBS is a longstanding illness with frequent abdominal discomfort and bowel symptoms that cannot be explained by any other disease. GI presentations include:
Abdominal pain or discomfort (present for at least 6 months) and relieved by defecation or associated with altered bowel frequency or stool form
Altered stool passage (straining, urgency, incomplete evacuation)
Abdominal bloating (more common in women than men)
Passage of mucus
IBS often also has extraintestinal features, including lethargy, nausea, back pain, headache or bladder symptoms. The condition rarely presents for the first time in people over 50 years old. The National Primary Care Diagnostic Pathway for Lower-GI Symptoms focuses on diarrhoea-predominant IBS (IBS-D).
The ROME criteria
A diagnosis of IBS can be supported by the ROME criteria.²⁵ Recurrent abdominal pain on average at least 1 day a week in the past 3 months, associated with two or more of the following criteria:
Related to defecation
Associated with a change in stool frequency
Associated with a change in stool form (appearance)
These criteria need to be fulfilled for the past 3 months, with symptom onset at least 6 months prior to diagnosis.
Quote goes here and here and here like this??
Making a diagnosis
IBS is a positive clinical diagnosis based on characteristic symptoms and normal initial investigations, rather than a diagnosis made only after excluding all other conditions.²⁶ ²⁷ A confident diagnosis of IBS can be made according to following symptoms:²⁸
Abdominal pain
Bowel dysfunction
Bloating
The diagnosis also requires exclusion of alarm symptoms, such as unintentional weight loss, rectal bleeding or recent change in bowel function, alongside normal haemoglobin (Hb), C-reactive protein (CRP), abdominal examination and digital rectal examination (DRE). Features not typical of IBS, such as nocturnal symptoms, iron deficiency anaemia, rectal bleeding or raised inflammatory markers, should prompt reconsideration of the diagnosis and further investigation. ²⁶ ²⁷
Coeliac disease
Coeliac disease occurs in 1-in-100 people and is undiagnosed in two-thirds of cases. It can present in non-specific ways, involving the common symptoms of lower-GI conditions described earlier, although potential distinguishing symptoms include:
Dermatitis herpetiformis
Tooth enamel problems
Reduced bone mineral density
Unexplained subfertility or repeated miscarriages
Neurological problems such as unexplained ataxia or peripheral neuropathy.
Coeliac UK focuses on fatigue, abdominal pain, nausea, anaemia and neurological symptoms as common symptoms and signs of coeliac disease in adults.²⁹ A 40-year single-centre analysis of 1547 found GI symptoms present in approximately half of coeliac patients, including:³⁰
Diarrhoea (24.3%)
Abdominal bloating (28%)
Aphthous stomatitis (19.7%)
Risk factors for Coeliac disease include:
Family history, with a first-degree relative associated with a 1-in-10 risk
Down's or Turner syndrome
History of autoimmune conditions (e.g. type 1 diabetes or thyroid disease)
Iron-deficiency anemia or B12 or folate deficiency.
Inflammatory bowel disease
IBD, which includes CD and UC, often presents with common lower-GI-symptoms, especially diarrhoea, abdominal pain, rectal bleeding or weight loss. Potential distinguishing symptoms include:
Nocturnal defecation
Fevers
Recurrent/persistent anal abscesses
Extra-intestinal manifestations (EIMs) in joints, skin, eyes or perianal area.
Perianal symptoms, such as fissures, abscesses or fistulae, may present early in CD, sometimes before intestinal symptoms.³¹⁻³³
IBD is classically considered as a disease of young adulthood, usually presenting in people aged 18–35 years. However, there is a second spike at around 65 years, with a large Swedish study showing 23% of IBD patients to be at least 60 years old at point of diagnosis.³⁴
Family history of IBD in a first-degree relative increases risk and should be considered during initial assessment.
Microscopic colitis
Microscopic colitis is a subset IBD distinct from CD or UD. The classical presentation is chronic watery non-bloody diarrhoea in older women (>60 years).³⁵ Others follow a similar pattern to lower-GI CD, with faecal urgency, arthralgias, weight loss, abdominal pain, passage of stools at night and faecal incontinence.³⁶ ³⁷ Microscopic colitis is associated with:
Autoimmune conditions, including coeliac disease, thyroid disorders and polyarthritis³⁵
Lifestyle factors, including smoking³⁸
Medications, including statins, selective serotonin reuptake inhibitors (SSRIs), proton-pump inhibitors (PPIs) and non-steroidal anti-inflammatory drugs (NSAIDs), with the latter two also associated with a rise in faecal calprotectin (FCP).³⁶
Microscopic colitis cannot be diagnosed in primary care.
Microscopic colitis is challenging to diagnose, as it appears macroscopically normal on endoscopy and requires histological confirmation by biopsy. A normal FCP result does not exclude a diagnosis (67% sensitivity; 75% specificity³⁹), so patients under high clinical suspicion should be referred for consideration of colonoscopy with biopsy. Many patients with undiagnosed microscopic colitis may have been through a diagnostic pathway with a colonoscopy already.³⁷
Around 10%⁴⁰ of microscopic colitis cases are self-limiting,⁴¹ but treatment with oral budesonide has been demonstrated to induce remission in between 54% to 84% of patients.⁴² Loperamide may be suggested for symptomatic relief; however, there is a limited evidence base for this and other treatments.
Extra-intestinal manifestations
IBD may have EIM (Table 2)s:⁴³ ⁴⁴
Dependent on the definition, the prevalence of EIMs is reported to be between 6% and 47% of all patients.⁴⁵
Patients may be affected by more than one EIM, with over 20% of IBD patients reporting two EIMs and over 10% of patients reporting three or more.⁴⁵
EIMs may occur before or after IBD diagnosis, with 26% of all patients with EIMs report occurrence of EIMs up to 25 months (median 5 months) before IBD diagnosis.⁴⁵
EIMs can precede bowel symptoms, so new uveitis, inflammatory back pain, erythema nodosum or peripheral arthritis alongside GI symptoms should raise suspicion for IBD.⁴⁵
In 25.8% of cases, patients presented with their first EIM before IBD was diagnosed (median 5 months, range 0–25 months), while In 74.2% of cases, the first EIM manifested itself after IBD diagnosis (median 92 months, range 29–183 months).⁴⁶
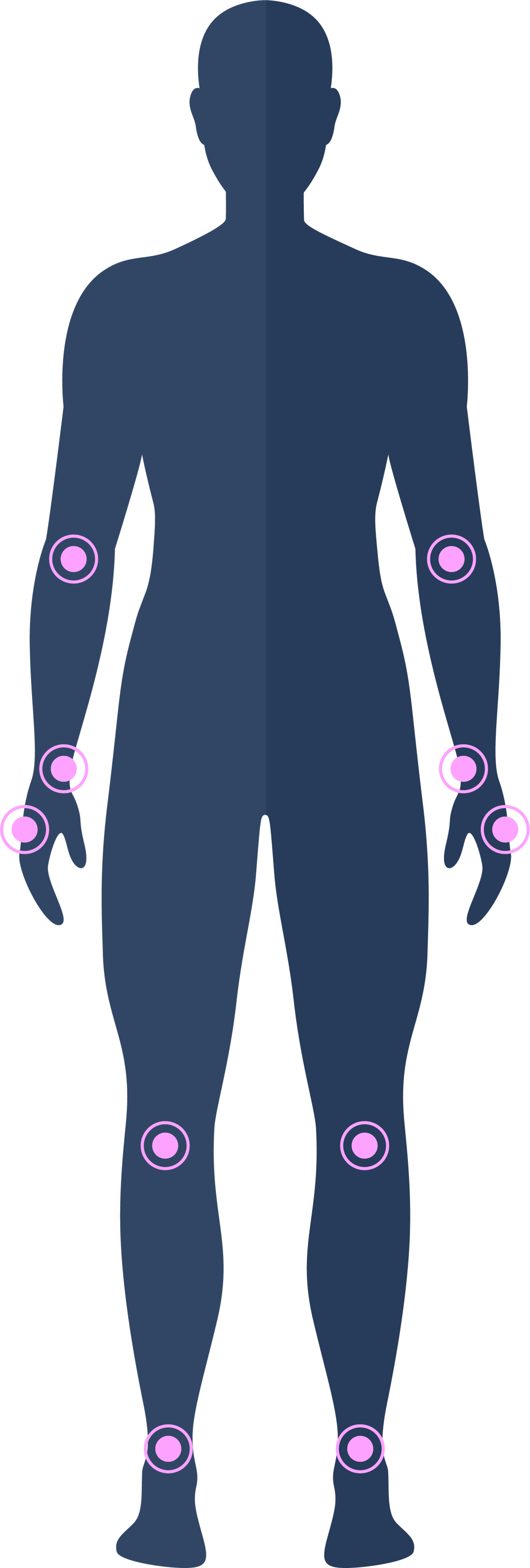
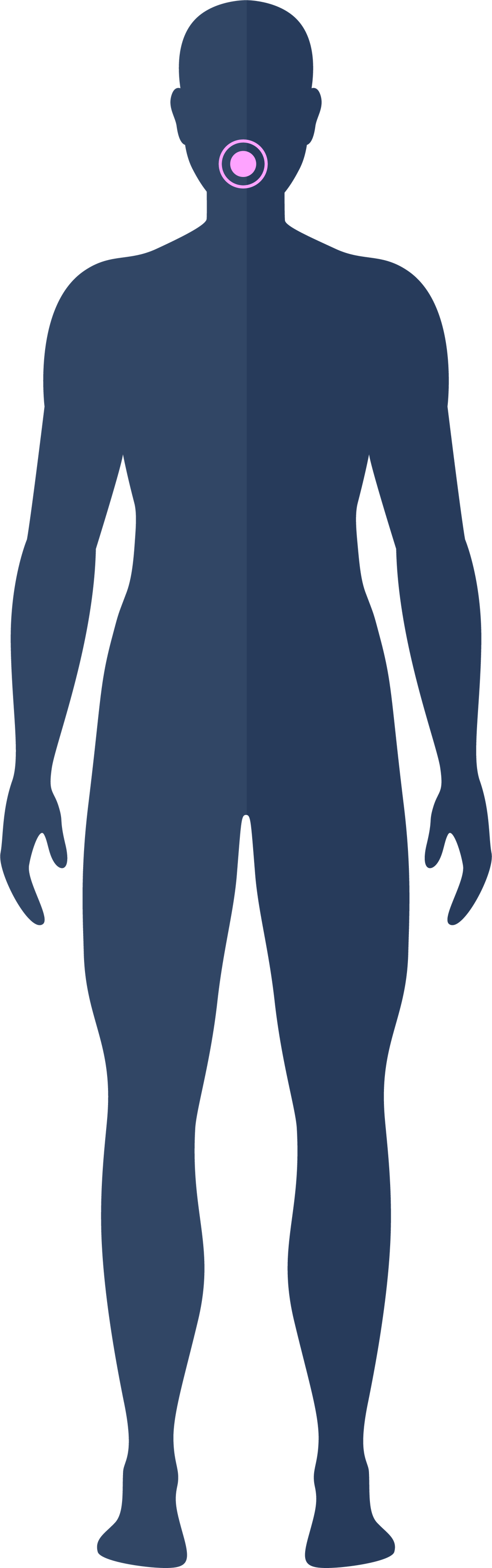
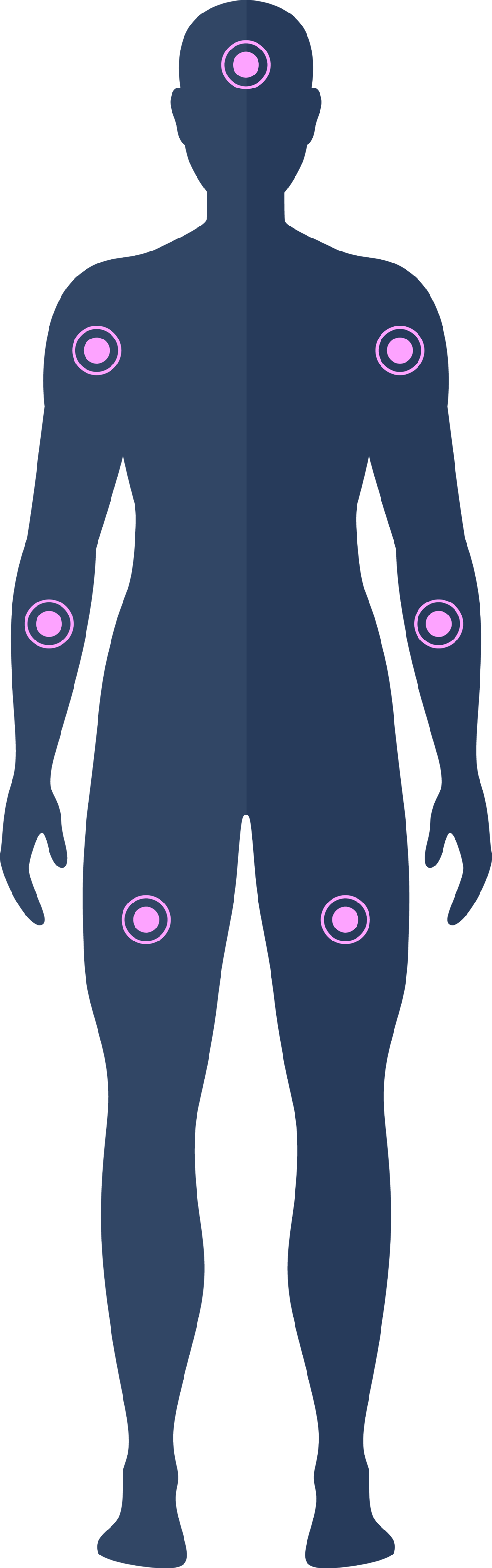
First extra-intestinal manifestations of inflammatory bowel disease⁴⁶
[Insert image below of the human body, hover over areas of the body to pull out incidence of different EIMs]46
Peripheral arthritis 70.0%
Aphthous stomatitis 21.6%
Axial arthropathy/ankylosing spondylitis 16.4%
Uveitis 13.7%
Erythema nodosum 12.6%
Primary sclerosing cholangitis 6.6%
Pyoderma gangrenosum 4.9%
Psoriasis 2.7%.
First extra-intestinal manifestations of inflammatory bowel disease⁴⁶
Peripheral arthritis 70.0%
Aphthous stomatitis 21.6%
Axial arthropathy/ankylosing spondylitis 16.4%
Uveitis 13.7%
Erythema nodosum 12.6%
Primary sclerosing cholangitis 6.6%
Pyoderma gangrenosum 4.9%
Psoriasis 2.7%.
Table 2. Extra-intestinal manifestations (%)⁴⁷ ⁴⁸
Manifestation
UC
UC
CD
CD
Peripheral arthritis
Axial arthritis
Anterior uveitis
Primary sclerosing cholangitis
4-14
≤20
3-4
≤5
10-20
≤50
5-12
-
Notes: Blank cells do not imply absence of this symptom in this condition, only absence of data in the cited studies.
HIV
HIV screening may be warranted in patients with GI symptoms, including chronic diarrhoea, depending on HIV stage:
Acute HIV infection in the first few weeks after exposure can include diarrhoea, nausea, fever, sore throat and muscle aches
Advanced HIV commonly includes persistent diarrhoea lasting more than a month, often linked to opportunistic infections.
Patients continue to be diagnosed late with HIV. Review of late diagnoses showed 62% had missed opportunities for diagnosis, of which 62% were in primary care. Of these patients, 82% presented with indicator conditions, which can include chronic diarrhoea.⁵⁰ GPs may miss opportunities to test for HIV due to:
Lack of knowledge of indicator conditions
Concern about causing offence to patient by suggesting an HIV test
Concern about consent required for test to be offered (minimum is seeking agreement to test and telling patient how result will be given).⁵¹


Patients continue to be diagnosed late with HIV. Review of late diagnoses showed 62% had missed opportunities for diagnosis, of which 62% were in primary care
?????
KNOWLEDGE CHECK
Question 1/4
Which statement about IBD in older adults is most accurate?

A – It is rare and usually long-standing from youth
B – It typically presents only with severe abdominal pain

C – It has a bimodal age distribution
Explanation: IBD has a recognised second peak in later life
D – It always causes raised FCP above 500
E – It is usually secondary to NSAID use
Go to next question
Question 2/4
Which feature most strongly suggests organic pathology rather than IBS?
A – Abdominal pain relieved by defecation
B – Bloating
C – Nocturnal diarrhoea
Explanation: Nocturnal symptoms are not typical of IBS
D – Symptom fluctuation
E – Association with stress
Go to next question
Question 3/4
Which combination most supports IBS diagnosis?
A – Weight loss and raised CRP
B – Nocturnal diarrhoea and anaemia
C – Abdominal pain relieved by defecation, normal CRP and low calprotectin
Explanation: Abdominal pain relieved by defecation, normal CRP and low calprotectin support an IBS diagnosis
D – Rectal bleeding and raised calprotectin
E – Persistent fever
Go to next question
Question 4/4
Which statement about IBS is most accurate?
A – It is a diagnosis only after colonoscopy

B – It is a disorder of gut–brain interaction
Explanation: IBS is a disorder of gut–brain interaction

C – It causes raised CRP
D – It requires lifelong laxatives
E – It is progressive
click for REFERENCES
What we focus on
Tools and features to help you move forward
We provide a few lightweight tools to help you focus, create, and adapt with clarity. Everything is built to work smoothly from the start, with just enough structure to support whatever you’re building.
01
Shapes turn into meaning
Some ideas begin without form. This helps give them just enough shape to move forward.
02
Space for what matters
Not everything needs to be filled. A bit of structure creates just the right amount of focus.
03
Movement without pressure
Progress doesn’t need to be loud. This is here to support a quiet, steady pace.
A digital learning tool designed to support primary care professionals in diagnosing lower-gastrointestinal symptoms using the national pathway.
www.crohnsandcolitis.org.uk